The Effects of Therapeutic Education on Self-care in Patients with Heart Failure and an Implantable Cardioverter Defibrillator: Study Protocol for a Randomised Controlled Trial
Angela Durante,1 Raúl Juárez-Vela,2 Michela Luciani,3 Sebastiano Marra,4 Ferdinando Varbella,5 Federica Rossi,6 Marta Giovannardi,7 Riccardo Sperlinga,8 Maria Michela Gianino9
1University of Rome Tor Vergata
2Universidad San Jorge Saragozza Spain
3Univeristy of Rome “Tor Vergata”, Research Nurse Department of Medicine and Surgery, University of Milano – Bicocca
4Cardiovascular Department, Città della Salute e della Scienza, University Hospital, Turin
5Cardiovascular Department, Rivoli Hospital, ASL TO3, Turin
6Carpi Hospital
7Cromsource srl
8Cattolica University, Turin
9Department of Public Health Sciences and Paediatrics, University of Turin.
Background
Heart failure (HF) is a clinical syndrome caused by an abnormality of the cardiac structure or function, leading to the heart’s failure to deliver oxygen at a rate commensurate with the requirements of the metabolizing tissues, despite normal filling pressures (or only at the expense of increased filling pressures).1 It is estimated that there are 23,000,000 people affected by HF worldwide, with approximately 2-3% in the European population.2 HF is a condition that increases in prevalence with age, and affects more than 25% of the population aged –84 years old. It has been predicted that by 2030 there will be an increase of 25% in the number of people with HF.3 In Italy, where this study will be conducted, the prevalence of HF is between 1.1% and 1.4% of the general population.4,5 Mortality due to HF is high after diagnosis: the 30-day, 1-year and 4-year mortality rates are 12.1%, 28.8% and 61.4%, respectively.9
To reduce the burden of HF, self-care is considered a cornerstone in HF treatment.6-22 In fact, it was shown in previous studies that HF patients who perform adequate self-care may have fewer hospitalizations, better QOL and even lower mortality.7,8 However, patients struggle to perform adequate self-care and it was found not at adequate levels in several studies.25,28
One of the main causes of death in patients with HF is sudden cardiac arrest due to ventricular arrhythmia.10,11 To prevent this problem, international guidelines suggest the implantation of an implantable cardiac defibrillator (ICD) in HF patients who are more exposed to sudden cardiac death: ICD therapy is associated with significant reduction in mortality compared with antiarrhythmic drug therapy.12-16
While an ICD implantation can lead to important clinical benefits (e.g., the 20% reduction of deaths), this procedure can also determine new clinical issues in HF patients and greater need of self-care behaviors.17,19 Since it has been already found that self-care is poor in HF patients,27 it is important that HF patients with ICD undergo educational intervention to improve their level of self-care.20,21
Study Objectives
The primary objective of this study will be to examine whether a nursing educational intervention based on therapeutic education can improve self-care in HF patients with recent implantations of ICD. The secondary objective will be to evaluate if a nursing educational intervention will improve quality of life in HF patients with ICD.
Methods / Design
Design of the study
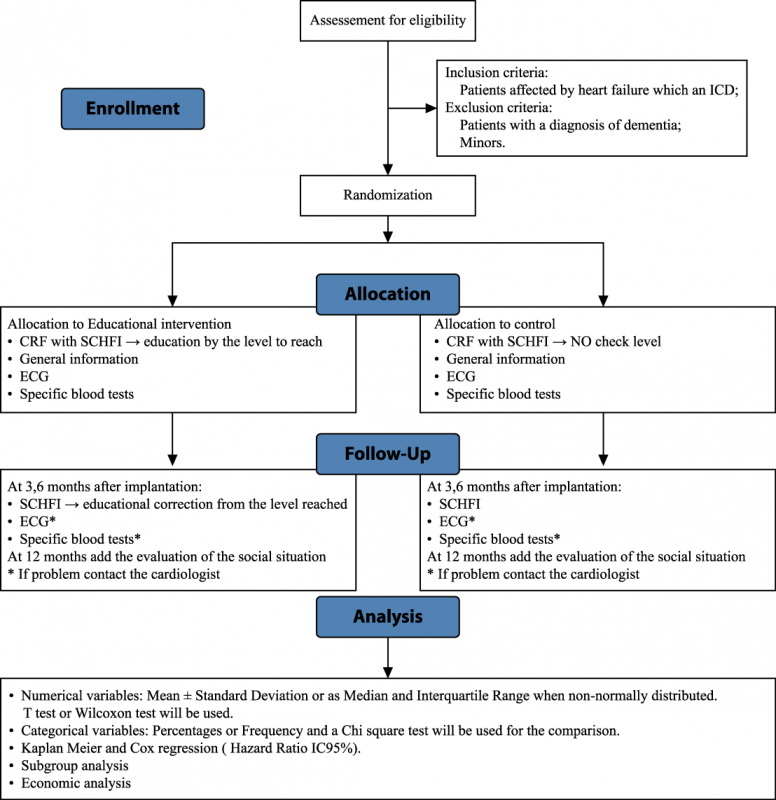
This is a multicenter, single blind, parallel-group study, which will involve two cardiovascular centers in northern Italy. The participant flowchart for the study is illustrated in Figure 1.
This study received formal ethical approval from both participating centers, ASLTO1 (Prot. 0123113) and ASLTO3 (Prot. 0006237 and Prot. 0008168).
Participants
The participants will be enrolled according to the following inclusion and exclusion criteria.
Inclusion criteria:
- Patients affected by HF according to the international guidelines, following elective hospitalization during which an ICD is implanted on an arrhythmic and/or ischemic basis.13,14,15
- Patients who provide written consent for this study. Exclusion criteria:
- Patients with compromised cognitive state with a diagnosis of dementia or Alzheimer disease.
- Minors: under the age of 18.
Instruments
HF patient self-care will be measured using the Self-Care of Heart Failure Index (SCHFI) version 6.2. This instrument consists of 3 scales: self-care maintenance, self-care management and self-care confidence. The self-care maintenance scale has 10 items, and measures how often the HF patient evaluates his/her symptoms (e.g., ankle swelling) and adheres to treatments (e.g., taking medications regularly). The self-care management scale has six items, and evaluates patient’s ability to recognize and evaluate the symptoms of HF exacerbation, implement a remedy to reduce symptoms (e.g., reducing fluid intake) and evaluate the effectiveness of the remedy if implemented. The self-care confidence scale has six items, and measures patient’s self-efficacy in all the self-care processes. Each scale uses a 4-point Likert scale for responses from “never or rarely” (1 point) to “every day or always” (4 points). The psychometric characteristics of the Italian version of the SCHFI v. 6.2 have been previously tested.28,29,31 Specifically, the instrument showed supportive fit indices at confirmatory factor analysis, and was able to discriminate patients educated in self-care versus those who were not. The test-retest reliability was also supportive, as was the internal consistency reliability. In all three SCHFI scales, a standardized score from 0 to 100 can be obtained, with a higher score meaning better self-care. A score of 70 or more is adequate self-care.7,30
Perceived quality of life in HF patients will be evaluated with a visual analogic scale (VAS). VASs are instruments with good validity and reliability to measure several variables including QOL.
The VAS that we will use consists of score from 0 to 100. The use is recommended in clinical trials to assess the global quality of life.32
For all the included patients, also the following data will be collected: socio-demographics (gender, age, educational level, marital status and country of birth), and clinical information (New York Heart Association (NYHA) functional classification, the implantation date, type of ICD, laboratory tests, ECG results and their changes at each follow-up and number of perceived shocks).33 The information on the patients’ diagnoses and possible associated diseases will be obtained through the analysis of clinical documentation, and will be collected in accordance with the International Statistical Classification of Diseases and Related Health Problems, 9th Revision (ICD-IX). Before any data collection, participants will be fully informed about the study and will be asked to sign the informed consent form.
Educational intervention
After randomization, all patients in the intervention group will undergo an educational intervention program, which will be delivered through a 30-minute talk given by the outpatient nurse during the first follow-up (7 ± 3 days from ICD implantation).23 The further educational interventions (3, 6 and 12 months) will be based on the SCHFI score obtained at the first follow-up. Specifically, a practical guide focused on HF self-care (e.g., recommending exercise) will be used with emphasis on the care of the surgical site where the ICD was implanted.34,35 The patients in the control group will receive the standard of care that is normally provided to HF patients after an ICD implantation.
Study outcomes and outcome measurements
The primary outcome of this study will include the self-care levels and their modifications measured using the SCHFI v. 6.2.24,26 The secondary outcomes will include the QOL. Also, we will evaluate the number of visits in the emergency department and hospitalization. All cause mortality 6 month after ICD implantation and the infection rate on the ICD device pocket.
The nurse at the outpatient clinic, in which the educational intervention will be conducted, will be able to consult the patient’s chart and research dossier. At the first follow-up, the nurse will proceed to gather socio-demographic and clinical data. During the first and subsequent follow-ups (at 7 ± 3 days and 3, 6 and 12 months), the self-care skills of the patients will be assessed using the SCHFI scale, and any changes in the previous data will be collected.
At the first follow-up visit and, if necessary, after 3 months, the nurse will assess the inflammatory signs and symptoms of the ICD pocket; if the signs increase, the patient will be asked to contact the hospital. The nurse will also assess the patient’s emergency department visits, hospitalizations, and the time spent by the patients and their companions; these will be checked at 3, 6 and 12 months. The research team will then investigate the databases of the clinical centers involved in this study, to gather information regarding hospitalizations and visits to the ED that occurred in the period between ICD implantation and the 12-month follow-up, as reported in the data collection files.
Sample size
The primary aim of this study was to examine the effects of a nursing educational intervention to improve the level of self-care, as measured through the SCHFI. A change in these scores is clinically relevant when the change is greater than half of one standard deviation from the mean;30 therefore, 128 patients (64 per group) with ICD implantations will be randomly assigned to the treatment or control groups. The sample size calculation was performed using Query Advisor software version 5.0, with a power of 80%.
Randomization
The “First Generator” software (available online at www.randomization.com) will be used to generate a randomization list, making it possible to assign participant to the intervention or control group.
Data analysis
The numerical variables will be reported as the mean ± standard deviation, or as the median and interquartile range when non-normally distributed. The t-test or non-parametric Wilcoxon test will be used, when appropriate, for the between-group comparisons. Normal distribution will be tested with the Kolmogorov Smirnoff test, and through the evaluation of the plot (plot of the data and q-q plot). The categorical variables will be expressed as a percentage or frequency, and a chi square test will be used for the comparison. The survival analysis will be evaluated through the Kaplan Meier analysis, and compared by the Log-Rank test. This solution involves conducting an intention-to-treat analysis. Furthermore, a Cox proportional hazards model will be implemented to assess the independent prognostic value of the educational program, adjusted for the variables significant in the univariable analysis. A hazard ratio (IC 95%) will be presented. In addition, the effects of the educational levels will be examined with regard to the perception of the quality of life in the different patient groups, according to specific characteristics (gender, age, NYHA class and level of education). For all of the statistical analyses, the significance will be set at p < 0.05. All of the analyses will be performed using the SAS 9.3 statistical package (SAS Institute Inc., Cary, NC, USA) and IBM SPSS Statistics version 22.
Discussion
The aim of this study will be to evaluate the effects of a nursing educational intervention on improving self-care in HF patients with recent ICD implantations. HF patients with ICDs are a growing and frail population that needs special attention from healthcare providers. Few studies have been conducted on self-care in HF patients with ICD, and we expect that because of the psychological problems experienced by this specific population, self-care will be poorer. Consequently, an intervention aimed at improving self-care will be particularly helpful for this specific population, and we anticipate that our study will improve self-care in HF patients with ICD. The participants in this study are expected to be compliant with the intervention and therapeutic education.
The majority of the medical demands today are concerned with chronic disease, and the health care providers can provide support to their patients with their life choices, and in helping them to improve the bio-psycho-social aspects of their health. In this regard, therapeutic education helps the patient to learn and develop numerous competencies, to adapt behaviors and improve different health parameters, including the bio-markers and quality of life. We also anticipate that therapeutic education in the intervention group will have an impact on costs. As demonstrated in the general HF population, patient education can be effective in reducing emergency department visits and hospitalizations.37,38,39 Consequently, we hypothesize that healthcare costs will decrease by the effect of the intervention.39
References
- McMurray JJ, Adamopoulos S, Anker SD, Auricchio A, Böhm M, Dickstein K, et al. ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail. 2012 Jul;33(14):1787-847.
- Rayney KJ. miR-155 in the heart: The Right Time at the Right Place in the Right Cell. Circulation. 2015 May 5;131(18):1533-5.
- Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Blaha MJ, et al. Heart Disease and Stroke Statistics -- 2014 update: A Report from the American Heart Association. Circulation. 2014:129(3): e28-e292.
- Valle R, Baccichetto R, Barro S, Calderan A, Carbonieri E, Chinellato M, et al. Heart Failure in Eastern Veneto: Prevalence, Hospitalization Rate, Adherence to Guidelines and Social Costs. Monaldi Arch Chest Dis. 2006;66(1):63-74.
- Gini R, Francesconi P, Mazzaglia G, Cricelli I, Pasqua A, Gallina P, Schuemie MJ. Chronic Disease Prevalence from Italian Administrative Databases in the VALORE Project: A Validation Through Comparison of Population Estimates with General Practice Databases and National Survey. BMC Public Health. 2013;13:15.
- Riegel B, Moser DK, Buck HG, Dickson VV, Dunbar SB, Lee CS, Lennie TA, Lindenfeld J, Mitchell JE, Treat-Jacobson DJ, Webber DE. Self-Care for the Prevention and Management of Cardiovascular Disease and Stroke: A Scientific Statement for Healthcare Professionals from the American Heart Association. J Am Heart Assoc. 2017 Aug 31;6(9).
- Lee CS, Bidwell JT, Paturzo M, Alvaro R, Cocchieri A, Jaarsma T, Strömberg A, Riegel B, Vellone E. Patterns of Self-Care and Clinical Events in a Cohort of Adults with Heart Failure: 1 Year Follow-Up. Heart Lung. 2017 Oct 17.
- Buck HG, Dickson VV, Fida R, Riegel B, D'Agostino F, Alvaro R, Vellone E. Predictors of Hospitalization and Quality of Life in Heart Failure: A Model of Comorbidity, Self-Efficacy and Self-Care. Int J Nurs Stud. 2015 Nov;52(11):1714-22.
- Ministry of Health of Italy http://www.salute.gov.it/portale/documentazione/p6_2_8_3_1.jsp? lingua=italiano&id=16. Accessed 11 Sept 2014.
- Gomez-Soto FM, Andrey JL, Garcia-Egido AA, Escobar MA, Romero SP, Garcia-Arjona R, Gomez F. Incidence and Mortality of Heart Failure: A Community-Based Study. International Journal of Cardiology. 2011;151(1):40-45.
- Stewart S, Ekman I, Ekman T, Oden A, Rosengren A. Population Impact of Heart Failure and the Most Common Forms of Cancer: A Study of 1,162,309 Hospital Cases in Sweden (1988 to 2004). Circ Cardiovasc Qual Outcomes. 2010;3(6):573-580.
- MacIntyre K, Capwell S, Stewart S, Chalmers JW, Boyd J, Finlayson A, et al. Evidence of Improving Prognosis in Heart Failure. Circulation. 2000;102:126.
- Hein J.J. Wellens, Peter J. Schwartz, Fred W. Lindemans, Alfred E. Buxton, Jeffrey J. Goldberger, Stefan H. Hohnloser, Heikki V. Huikuri, Stefan Kääb, Maria Teresa La Rovere, Marek Malik, Robert J. Myerburg, Maarten L. Simoons, Karl Swedberg, Jan Tijssen, Adriaan A. Voors, Arthur A. Wilde European Heart Journal May 2014, ehu176; DOI: 10.1093/eurheartj/ehu176
- Villacastin J, Bover R, Castellano N. P, Moreno J, Morales R, Garcia-Espinosa A. Risk Stratification and Prevention of Sudden Death in Patients with Heart Failure. Rev Esp Cardiol. 2004;57:768-82.
- Merkely B, Kautzner J, Milasinovic G, Hatala R, Taborsky M, Lubinski A et al. EHRA, Summit 2010. Summary Statement: EHRA Summit 2010 with the Participation of Central-Eastern European Countries: ‘ICD for Life’ Initiative –Fighting Against Sudden Cardiac Death in Emerging Economies. Europace 2011;13:1209–10.
- Willich, T., and A. Goette. "Update on Management of Cardiac Arrhythmias in Acute Coronary Syndromes." Minerva Cardioangiologica 63.2 (2015): 121-133.
- Brouwers C, Caliskan K, De Jonge N, Theuns D, Costantinescu A, Young QR, et al. A Comparison of the Health Status and Psychological Distress of Partners of Patients with a Left Ventricular Assist Device Versus an Implantable Cardioverter Defibrillator: A Preliminary Study. Heart & Lung: The Journal of Acute and Critical Care. 2015;44(1):27-32.
- Wong F.M.F., Sit J.W.H., Wong E.M.L. & Choi K.C. (2014) Factors Associated with Health-Related Quality of Life Among Patients with Implantable Cardioverter Defibrillator: Identification of Foci for Nursing Intervention. Journal of Advanced Nursing 70(12), 2821–2834. doi: 10.1111/jan.12434.
- Lang, S., Becker, R., Wilke, S., Hartmann, M., Herzog, W., & LÖWe, B. (2014). Anxiety Disorders in Patients with Implantable Cardioverter Defibrillators: Frequency, Course, Predictors, and Patients' Requests for Treatment. Pacing & Clinical Electrophysiology, 37(1), 35-47. doi:10.1111/pace.12276.
- Jourdain P, Juillière Y, Steering and Working Group Committee Members of the French Task Force on Therapeutic Education in Heart Failure. Therapeutic Education in Patients with Chronic Heart Failure: Proposal for a Multiprofessional Structured Programme. Arch Cardiovasc Dis. 2011 Mar;104(3):189-201.
- World Health Organization Regional Office for Europe. Therapeutic Patient Education Continuing Education Programmes for Health Care Providers in the Field of Prevention of Chronic Diseases. Copenhagen: WHO Regional Office for Europe; 1998.
- Gallacher K, May CR, Montori VM, Mair FS. Understanding Patients' Experiences of Treatment Burden in Chronic Heart Failure Using Normalization Process Theory. Annals of Family Medicine. 2011;9(3):235-243.
- Prochaska JJ, Hall S, Delucchi K, Hall SM. Efficacy of Initiating Tobacco Dependence Treatment in Inpatient Psychiatry: A Randomized Controlled Trial. American Journal of Public Health. 2013. doi:10.2105/AJPH.2013.301403.
- Stroi:10. A. Educating Nurses and Patients to Manage Heart Failure. Eur J Cardiovasc Nurs. 2002;1:33-40.
- Johnson SS, Driskell MM, Johnson JL, Dyment SJ, Prochaska JO, Prochaska JM, et al. Transtheoretical Model Intervention for Adherence to Lipid-Lowering Drugs. Disease Management. 2006a;9:102-114.
- Johnson SS, Driskell MM, Johnson JL, Prochaska JM, Zwick W, Prochaska JO. Efficacy of a Transtheoretical Model-Based Expert System for Antihypertensive Adherence. Disease Management. 2006b;9:291-301.
- DORS. Modelli socio cognitivi per il cambiamento dei comportamenti: Rassegna e analisi critica. 2009. http://www.dors.it/alleg/0202/Modelli%20teorici%20di%20cambiamento2.pdf. Accessed 14 Oct 2014.
- Cocchieri A, Riegel B, D'Agostino F, Rocco G, Fida R, Alvaro R, Vellone E. Describing Self-Care in Italian Adults with Heart Failure and Identifying Determinants of Poor Self-Care. Eur J Cardiovasc Nurs. 2014;9.
- Vellone E, Riegel B, Cocchieri A, Barbaranelli C, DC, Dranel F, Antonetti G, et al. Psychometric Properties of the Self-Care of Heart Failure Index Version 6.2. Res Nurs Health. 2013;36:500-511.
- Riegel B, Lee CS, Dickson VV, Carlson B. An Update on the Self-Care of Heart Failure Index. J Cardiovasc Nurs. 2009;24:485-497.
- Pulignano G, Del Sindaco D, Minardi G, Tarantini L, Cioffi G,Bernardi L, et. al. Translation and Validation of the Italian Version of the European Heart Failure Self-Care Behaviour Scale. Federazione italiana di cardiologia. Eur J Cardiovasc Med. 2010;11:493-498.
- De Boer AG, Van Lanschot JJB, Stalmeier PF, Van Sandick JW, Hulscher JB, De Haes JC, et al. Is a Single-Item Visual Analogue Scale as Valid, Reliable and Responsive as Multi-Item Scales in Measuring Quality of Life? Quality of Life Research. 2004;13(2):311-320.
- Aspromonte N, Di Tano G, Lantini R, Masson S, Valle R, Emdin M. Ruolo dei biomarcatori per la stratificazione prognostica e la personalizzazione del follow-up nel paziente con scompenso cardiaco. G Ital Cardiol. 2010;11(5 Suppl. 2):17S-23S.
- Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE, Drazner MH, et al. 2013 ACCF/AHA Guideline for the Management of Heart Failure: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;62:147-239.
- Epstein AE, Di Marco J, Ellebogen KA, Estes M, Freedman RA, Gettes LS, et al. American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society Report of Guidelines for Implantable Defibrillator and Cardiac Resynchronization Therapy for Cardiac Rhythm Abnormalities, 2012.
- Government of Western Australia Department of Health. Traffic light criteria. http://www.healthyoptions.health.wa.gov.au/visitors/traffic_light.cfm. Accessed 7 Oct 2014.
- Jackevicius CA, De Leon NK, Lu L, Chang DS, Warner AL, Mody FV. Impact of a Multidisciplinary Heart Failure Post-Hospitalization Program on Heart Failure Readmission Rates. Ann Pharmacother. 2015 Aug 10.
- Kalista T, Lemay V, Cohen L. Postdischarge Community Pharmacist-Provided Home Services for Patients after Hospitalization for Heart Failure. J Am Pharm Assoc (2003). 2015 Jul-Aug;55(4):438-442.
- Yu M, Chair SY, Chan CW, Choi KC. A Health Education Booklet and Telephone Follow-Ups Can Improve Medication Adherence, Health-Related Quality of Life, and Psychological Status of Patients with Heart Failure. Heart Lung. 2015 Sep-Oct;44(5):400-407.